Cardiovascular disease (CVD) is the leading cause of death among women worldwide, surpassing all forms of cancer combined. Yet, for decades, CVD has been perceived as a predominantly male disease, leading to significant gaps in awareness, diagnosis, prevention, and treatment for women. While overall CVD mortality rates have declined due to advances in medicine, this progress has not been evenly distributed—especially among younger women and women of color.
Women’s cardiovascular risk is uniquely influenced by hormonal transitions, pregnancy-related complications, autoimmune conditions, and psychosocial factors such as chronic stress and caregiving burdens. Furthermore, clinical symptoms of CVD in women often differ from the “classic” male presentation, contributing to delays in diagnosis and worse outcomes.
This article explores the clinical nuances of cardiovascular risk in women and provides evidence-based nutritional and lifestyle strategies tailored to the female lifespan. By integrating sex-specific insights into prevention, healthcare providers and individuals can more effectively reduce cardiovascular burden in women and promote lifelong vascular health.
Understanding the Gender Gap in Cardiovascular Risk
Historically, women have been underrepresented in cardiovascular research, leading to a male-centric understanding of disease presentation and progression. This has contributed to disparities in outcomes. Women are more likely to experience:
- Atypical symptoms (e.g., fatigue, nausea, shortness of breath)
- Misdiagnosis or delayed diagnosis
- Less aggressive treatment for acute coronary syndromes
Female-Specific Risk Factors
Hormonal Shifts Across the Lifespan
- Estrogen has vasodilatory and lipid-modulating effects. Its decline during menopause is associated with increased LDL cholesterol, insulin resistance, and endothelial dysfunction.
- Early menopause (<45 years) is independently linked to higher CVD risk.
Pregnancy-Related Complications
- Preeclampsia, gestational diabetes, and hypertensive disorders of pregnancy are strong predictors of future hypertension and ischemic heart disease.
- These conditions are now considered “early-life stress tests” for cardiovascular function.
Autoimmune Diseases
- Women are disproportionately affected by SLE and rheumatoid arthritis, both of which accelerate atherosclerosis via chronic inflammation.
Polycystic Ovary Syndrome (PCOS)
- Associated with hyperinsulinemia, dyslipidemia, and central obesity—major components of metabolic syndrome.
Dietary and Lifestyle Strategies for Prevention
Preventing cardiovascular disease in women requires a comprehensive approach that addresses both the physiological differences unique to women and modifiable lifestyle factors. Nutrition and physical activity are powerful tools for reducing inflammation, controlling risk factors, and supporting vascular integrity across all life stages.
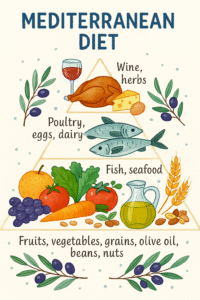
1. Adopt a Mediterranean Diet
- Key components: Extra virgin olive oil, leafy greens, legumes, fish (esp. fatty fish like salmon), nuts, whole grains, and red wine in moderation.
- Cardioprotective effects: Improves endothelial function, reduces LDL oxidation, lowers blood pressure, and reduces systemic inflammation.
🧠 Clinical Insight: A meta-analysis by Estruch et al. (2013) demonstrated a 30% reduction in major cardiovascular events among high-risk individuals adhering to this diet.
2. Follow the DASH Diet
- Emphasis: High potassium (fruits/vegetables), low sodium, lean proteins, low-fat dairy, and whole grains.
- Clinical goal: Manage or prevent hypertension, maintain vascular elasticity, and reduce stroke risk.
3. Balance Omega-3 and Omega-6 Fatty Acids
- Sources of EPA/DHA: Fatty fish, fish oil supplements.
- Clinical relevance: Omega-3s have been shown to reduce arrhythmias, lower triglyceride levels, and reduce clot formation.

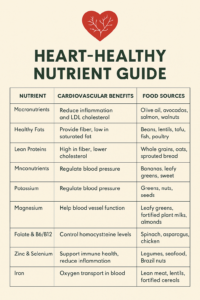
4. Optimize Micronutrient Intake
| Nutrient | Benefits for Women |
|---|---|
| Magnesium | Improves insulin sensitivity and relaxes blood vessels |
| Potassium | Offsets sodium, critical for blood pressure control |
| Calcium & Vitamin D | Bone protection + may modulate vascular tone |
| Folate, B6, B12 | Reduce homocysteine levels linked to atherogenesis |
| Antioxidants (e.g., flavonoids) | Protect against oxidative vascular damage |
5. Reduce Pro-Inflammatory and Atherogenic Foods
- Limit: Processed meats, sugary drinks, refined carbohydrates, trans fats, and excess alcohol.
- These foods increase LDL, disrupt glucose metabolism, and promote systemic inflammation—accelerating atherosclerosis.
Life Stage–Focused Prevention (Expanded)
Recognizing the hormonal and physiological transitions that occur throughout a woman’s life is essential to tailoring prevention efforts effectively.
Adolescence and Young Adulthood (15–40 years)
Goals: Establish healthy habits early, address emerging metabolic risks, and screen high-risk groups (e.g., family history, PCOS, obesity).
- Encourage physical activity ≥150 minutes/week
- Emphasize menstrual cycle regularity as a cardiometabolic indicator
- Screen for insulin resistance or lipid issues in women with PCOS
- Promote iron-rich and heart-healthy diets (e.g., leafy greens, legumes, fortified whole grains)
Perimenopause and Early Postmenopause (40–55 years)
Goals: Manage vasomotor symptoms and increased central adiposity; mitigate the steep rise in LDL, BP, and glucose resistance that occurs with estrogen decline.
- Annual assessments: BP, lipids, glucose, waist circumference
- Promote Mediterranean-style diet and strength/resistance training to preserve muscle mass
- Consider adding soy isoflavones or flax (plant-based phytoestrogens) for mild hormonal support
- Limit sodium and processed foods to control blood pressure and bloating
🧠 Clinical tip: Hot flashes and night sweats may correlate with early vascular changes—use them as a cue to intervene preventively.
Late Postmenopause (55+ years)
Goals: Address aging-related declines in muscle mass, increasing arterial stiffness, and compounded risk factors like osteopenia, diabetes, and hypertension.
- Prioritize anti-inflammatory foods to reduce CVD and dementia risk
- Monitor for silent ischemia, more common in older women
- Nutrient supplementation may be necessary (vitamin D, B12, magnesium)
- Encourage social and mental well-being as part of CVD prevention (e.g., walking groups, cognitive training)
👵 Note: Depression is both a consequence and risk factor for CVD in aging women—early psychological support can be protective.

Final Takeaway
Cardiovascular prevention in women must go beyond generic advice. Clinicians should consider gender-specific risk factors, tailor dietary interventions, and support behavior change across every stage of life. With a proactive, prevention-focused approach, the trajectory of CVD in women can be dramatically altered.
Next in the Prevention Series:
Preventing Cognitive Decline and Vascular Dementia – exploring the vascular-brain connection and neuroprotective nutrition.
References:
- Ross, A. C., Caballero, B., Cousins, R. J., Tucker, K. L., & Ziegler, T. R. (2014). Modern Nutrition in Health and Disease (11th ed.). Lippincott Williams & Wilkins.
- Berdanier, C. D., & Berdanier, L. A. (2021). Advanced Nutrition: Macronutrients, Micronutrients, and Metabolism (3rd ed.). CRC Press.
- Frayn, K. N. (2010). Metabolic Regulation: A Human Perspective (3rd ed.). Wiley-Blackwell.
- Combs, G. F., & McClung, J. P. (2022). The Vitamins: Fundamental Aspects in Nutrition and Health (6th ed.). Elsevier.
- Libby, P. (2021). The changing landscape of atherosclerosis. Nature, 592(7855), 524–533. https://doi.org/10.1038/s41586-021-03392-8
- Mosca, L., Benjamin, E. J., Berra, K., et al. (2011). Effectiveness-based guidelines for the prevention of cardiovascular disease in women—2011 update. Circulation, 123(11), 1243–1262. https://doi.org/10.1161/CIR.0b013e31820faaf8